

DISCUSSING NEURODIVERSITY

Neurodiversity is a term that was coined by Australian sociologist Judy Singer in 1998 which has become an integrated term in neuroscience and psychology.
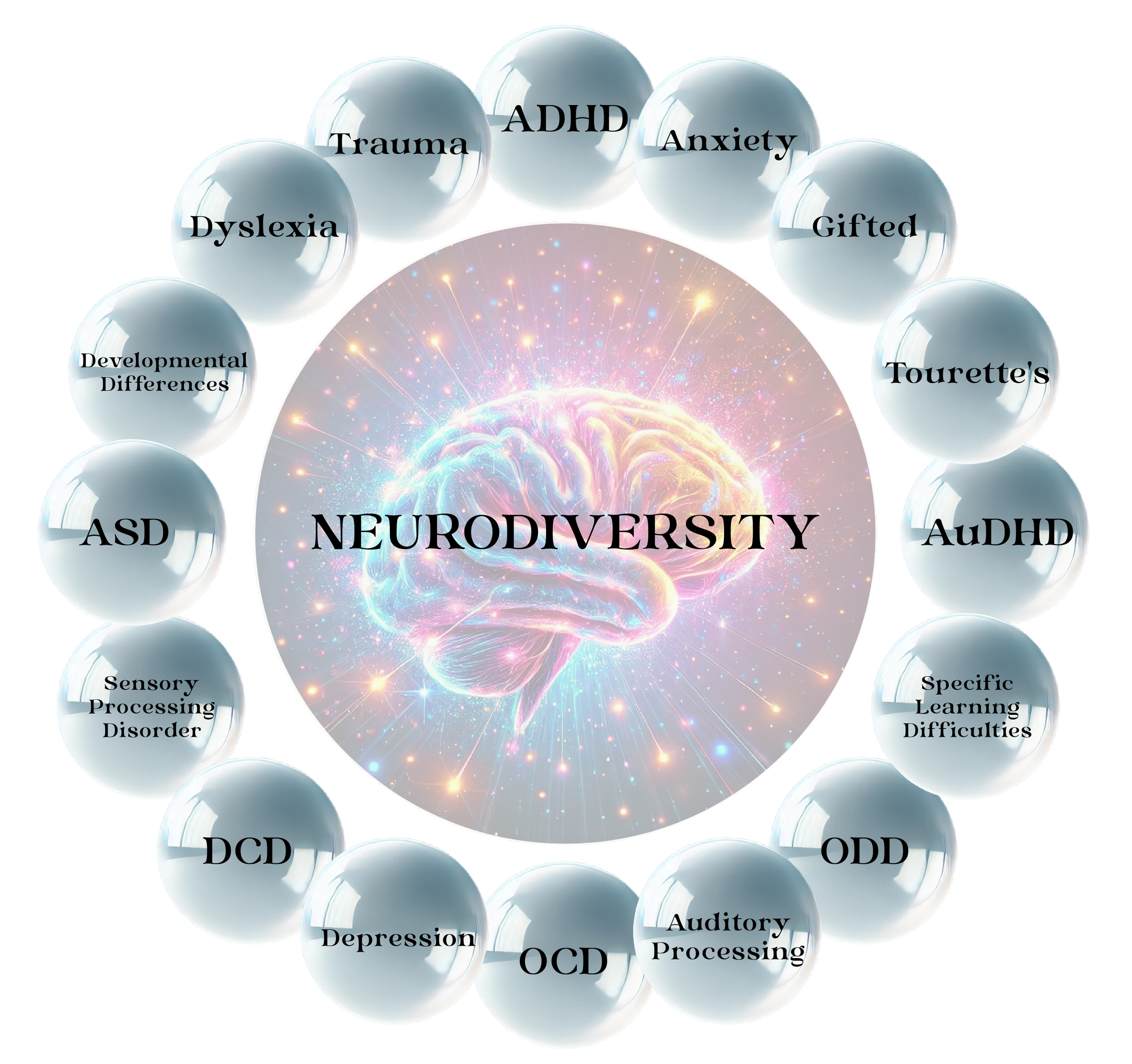
‘Neurodiversity’ means that everyone’s brain works in unique ways. The term recognises that certain diagnosed differences in how people think, learn, and experience the world are natural parts of human diversity. These neurodiverse diagnoses include ASD (Autism Spectrum Disorder - formally Asperger’s and Autism), ADHD (Attention Deficit Hyperactivity Disorder), AuDHD (a combined diagnosis of ADHD and ASD), Dyslexia, and many other neurodevelopmental variations and adjacent diagnoses. This umbrella of diagnoses is regularly updated as research develops and new editions of Diagnostic Manuals, such as the DSM (currently the DSM-5) are released. Many neurodivergent conditions are shown in this graphic, however, it may not be complete.
Neurodiversity as a term recognises that these differences are not problems to be solved, but celebrations of neurological variations that contribute to the richness and creativity of our society.
Below, we explore ADHD, AuDHD, and ASD so that the differences and similarities of these diagnoses can be seen.
WHAT IS NEURODIVERSITY?
ADHD - Attention Deficit Hyperactivity Disorder
AuDHD - A combined diagnosis of ADHD and ASD
ASD - Autism Spectrum Disorder (formerly encompassing Asperger’s and Autism)
DCD - Developmental Co-ordination Disorder
ODD - Oppositional Defiance Disorder
OCD - Obsessive Compulsive Disorder
“Neurodiversity may be the birthplace of some of humanity’s greatest minds.”
— Harvey Blume
ADHD (Attention Deficit Hyperactivity Disorder) is a lifelong neurodevelopmental condition people are born with and is characterised by a variety of traits that affect everyday life. It has a hereditary component, and symptoms are present from early development. It is lifelong and is not something someone grows out of, although traits and characteristics can change in severity throughout a person's life. Diagnosis is made by qualified specialists, commonly psychiatrists, paediatricians, or clinical psychologists, though only medical doctors, such as psychiatrists, paediatricians etc, can prescribe medication.
Traits included in this diagnostic criteria look for specific issues around inattention, hyperactivity in body and/or thinking, and impulsivity. There are many other common traits that people diagnosed with ADHD share, however, such as difficulties with executive functioning, memory issues, distraction, hyperfocus, hypofocus, and more. Unfortunately, self-esteem problems are also common in ADHD, however, not a feature of the diagnosis. Rather, these self-esteem issues arise from experiences where traits are often misunderstood or undervalued, meaning ADHDers are often criticised as rude, lazy and weird. Low self-esteem is therefore ‘learned’ from prolonged exposure to negative feedback in one's environment. Individuals may eventually internalise these comments and believe them to be accurate, leading to negative self-talk.
ADHD traits can impact a person in all environments, including home, social situations, school, and work. In the past, terms like ‘ADD’ were used, but now all variants are diagnosed under ADHD with different presentation types. These types, according to the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) and ICD-11 (International Classification of Diseases, Eleventh Edition), are:
ADHD-I (Predominantly Inattentive Type) - people struggle primarily with focus and attention, and can find focusing on tasks difficult. They are easily distracted and can be forgetful and have poor organisational skills, often misplacing things or failing to follow through on tasks. Can have issues keeping spaces tidy and can sometimes be seen as ‘daydreamers’.
ADHD-H (Predominantly Impulsive/Hyperactive Type) - people struggle primarily with impulsivity and high levels of physical and mental activity. Often need to move or fidget and talk excessively, often interrupting others to ‘get it out’ before they forget. Often make quick decisions without thinking them through, and can be seen as ‘disruptive’.
ADHD-C (Combined Type) - people exhibit a mixture of both inattentive and impulsive/hyperactive type symptoms equally. Combined type ADHDers will exhibit both difficulties with focusing and attention, as well as impulsivity and high levels of physical and mental activity.
ADHD
AuDHD
AuDHD is not an official term, but one coined and used by the Neurodiverity Community and support groups to identify someone as having both an ADHD and an ASD diagnosis. It was not until the DSM-5 was published in 2013 that a person could be diagnosed with both ADHD and ASD. Prior to that, if a person was diagnosed with one ‘disorder’, they were locked out of being tested and diagnosed with the other. We now know that it is not only possible to have both ADHD and ASD diagnoses in one person, but that the symptoms and difficulties faced by a person diagnosed as AuDHD are distinct from those who are diagnosed as ADHD or ASD alone. This reflects the common co-occurrence of neurodevelopmental, mental health, and physical health conditions seen within neurodiversity. It’s uncommon for a neurodivergent person to experience only a single condition, and research shows that a neurodivergent diagnosis means it is extremely likely that there will be the discovery of additional diagnoses.
AuDHD is a new field of research, and trying to find statistics on the exact numbers of AuDHD incidence in people diagnosed with ADHD or ASD differs greatly. As of late 2025, it is thought that 20% - 50% of people diagnosed with ADHD also subsequently received a diagnosis of ASD, and that 40% - 70% of people diagnosed with ASD also subsequently received a diagnosis of ADHD. Once both diagnoses are applied, many use the term AuDHD, no matter which diagnosis came first. Dr Khurram Sadiq, a consultant neurodevelopmental psychiatrist in London, who himself has an AuDHD diagnosis, is a leading researcher into AuDHD. His findings so far have led him to presume there is a 50% - 70% co-occurrence of ADHD and ASD diagnoses overall*.
A person with AuDHD will show traits of both ADHD and ASD, however, as traits are conflicting in these conditions, many diagnosed with AuDHD also suffer from anxiety and will ‘mask’ many behaviors when interacting with society. This combination of ADHD and ASD can create distinct experiences, for example, feeling a strong urge to plan yet struggling to carry tasks out, or relying on routine for comfort while also experiencing sudden boredom and craving novelty or excitement. This internal push-and-pull often heightens anxiety, with emerging research indicating that the overlap of these traits may contribute to even greater anxiety within AuDHD individuals than those diagnosed with ADHD or ASD alone. Like ADHD, individuals with AuDHD often suffer from low self-esteem due to traits being misunderstood within neurotypical society and external criticism becoming negative internal self-talk.
An AuDHDer receiving a diagnosis of just ADHD or ASD before 2013 could exacerbate feelings of negative self-esteem, as traits of one condition or the other did not fully encompass the lived experience of a person with AuDHD. Although more is being discovered around AuDHD and its individual differences of neurobiology and behaviour, it is still a new field with many diagnosed with the condition adding to the understanding of how it differs as a neurodiverse diagnosis.
* (Sadiq, 2025)
TikTok by @speechdude
ASD
Autism Spectrum Disorder (ASD) is a lifelong neurodevelopmental condition that encompasses what were previously separate diagnoses, including Autistic Disorder and Asperger’s Syndrome. The word ‘spectrum’ reflects the wide variation in how ASD presents from person to person, in both strengths and challenges. ASD is present from birth, has a hereditary component, and involves differences in social interaction, communication, and patterns of restricted or repetitive behaviours, interests, or activities. The DSM-5 classifies ASD into Levels 1–3, referring to the degree of everyday support a person may require.
To receive a diagnosis, an individual must show persistent differences in two core areas:
Social communication and interaction, and
Restricted or repetitive behaviours and interests.
In Australia, ASD can be diagnosed by qualified professionals such as paediatricians, psychologists, or psychiatrists—often within a multidisciplinary team that may also include speech pathologists or occupational therapists. The process typically begins with a referral from a GP or local doctor.
Social communication and interaction differences may include unusual or limited eye contact, difficulty interpreting body language and facial expressions, or speaking with an atypical tone. Some individuals may find it challenging to initiate or sustain conversations, or may prefer to talk primarily about a narrow range of interests.
Restricted and repetitive behaviours, interests, or activities might include forms of stimming such as hand-flapping, rocking, inner-mouth chewing, skin picking, spinning, or repeating words, songs, or phrases (echolalia). Many ASD people experience discomfort or distress with unexpected changes to routines or environments and often prefer predictability. Sensory differences are common, with individuals experiencing heightened or reduced sensitivity to sound, light, touch, taste, or smell. Deep or highly specialised interests are also characteristic.
When people hear the word “autism” in everyday conversation, they often imagine someone with high support needs (Level 3), a perception influenced by film and television portrayals. Meanwhile, individuals with Level 1 ASD, previously referred to as Asperger’s, are frequently misunderstood or labelled as “quirky,” “stubborn,” or “odd” as they do not display the same degree of ‘autistic’ traits seen in Levels 2 and 3. Such misunderstandings, particularly during childhood and schooling, can contribute to self-esteem difficulties and social challenges. Anxiety is also a common co-occurrence in all Levels of ASD, as navigating social cues and others’ perspectives can be confusing or overwhelming, leading many ASD people to mask their natural behaviours to fit in. Stimming can act as an important self-soothing strategy, especially in stressful situations.
It is also worth noting that people with ADHD and those who are AuDHD often stim, use echolalia, and experience sensory sensitivities, as these neurodevelopmental conditions can overlap in how they affect communication, regulation, and perception.

MASKING
Masking, sometimes called camouflaging, is a coping strategy in which neurodivergent people, most often associated with ADHD, ASD or AuDHD, intentionally or unintentionally hide their natural behavioural traits and tendencies to blend in with neurotypical social expectations and situations. It’s a learned behaviour as a form of self-protection, and it usually develops in a person from a young age in the desire to be accepted socially or to look ‘normal’. Neurodivergent people mask in an effort to avoid stigma, bullying, or discrimination.
Whether conscious or unconscious, masking is emotionally and physically tiring and can lead to high levels of anxiety. Masking is well known to occur in ASD, however, ADHD and AuDHD also mask behavioural traits for social acceptance from a young age. Like ASD, an ADHD/AuDHD person often experiences negative backlash throughout childhood and beyond for behavioural traits instinctive to them, meaning that they try to minimise or change their way of behaving and thinking to fit into neurotypical society.
A NOTE ON MEDICATION
Medication is commonly prescribed for individuals diagnosed with ADHD. These medications are most often stimulants, although non-stimulant medications can be used when a person experiences side effects from stimulants or has other medical conditions that make stimulants unsuitable. Stimulant medications increase certain neurotransmitters in the brain, which helps improve focus, attention, and the ability to regulate behaviour. Both short-acting and long-acting formulations exist to suit different needs and lifestyles.
Because of their impact on concentration, stimulants are frequently used by students and adults who need sustained attention in education or the workplace. Even long-acting stimulants do not necessarily need to be taken every single day. In consultation with a health professional, some people choose to use them only on days when higher levels of focus are required, for example, Monday to Friday rather than on weekends.
Non-stimulant ADHD medications work differently and tend to have a slower onset, but they also aim to improve attention and focus. Some stimulant and non-stimulant medications can also help with impulsivity. Medication plans are tailored to each individual and their particular ADHD traits, challenges, and daily demands.
There is no equivalent medication that treats the core traits of ASD. Instead, support tends to be therapy-based, such as behavioural interventions, skill-building, and coaching. However, many individuals with ASD, ADHD, or AuDHD are prescribed SSRIs (Selective Serotonin Reuptake Inhibitors) to treat co-occurring conditions like anxiety, depression, and certain types of repetitive or distress-related behaviours. SSRIs typically need to be taken daily and require close monitoring by a healthcare professional, just as stimulant medications do.
Within the AuDHD community, people often discuss how medications affect the interplay between ADHD and autistic traits. Some report that taking stimulants seems to “turn down” the ADHD symptoms, making their autistic traits feel more noticeable. These observations are based on community experiences rather than formal research at this stage.
Medication is not mandatory for ADHD, and each person should work with their healthcare professional to decide what is most effective and appropriate. Many adults also use lifestyle adjustments, such as changes to routines, sleep, diet, exercise, and environment, to support their neurodivergent needs. Therapy, coaching, and some complementary approaches (such as acupuncture, chiropractic care, or massage) may also provide additional support, depending on individual preference.
It is essential that any prescription medication is discussed thoroughly with a qualified health professional, and that decisions about starting, stopping, or changing medication are made collaboratively. Never adjust medication without professional guidance.
A NOTE ON GIRLS & WOMEN
Historically, ADHD was viewed largely as a boys’ condition, partly because the signs often present differently in biological females than in males. Studies conducted between 1987 and 1994 included predominantly male participants, over 80%, and it wasn’t until the late 1990s that research began to focus more intentionally on gender differences in ADHD presentation. Several factors contributed to this imbalance, including longstanding male bias in medical research, the perception that behaviours like hyperactivity are typical for boys but inappropriate for girls, and the tendency to interpret inattentive symptoms in girls as daydreaming rather than neurodivergence. Broader societal expectations about what is considered normal or acceptable behaviour for boys versus girls in school settings further reinforced these disparities.
As a result, many biological females with ADHD who grew up in the 1980s and 1990s were overlooked, labelled as having behavioural issues, or misdiagnosed, most often with anxiety or depression. Today, the largest group of newly diagnosed women are those receiving a “late” diagnosis, meaning they seek formal diagnosis in adulthood, often in their thirties, forties, or beyond.
A significant number of these late-diagnosed women discover their neurodivergence while seeking assessments for their children. During the diagnostic process, they recognise similar traits in themselves and subsequently pursue their own diagnosis. This pattern can occur for fathers as well, as ADHD has a strong hereditary component.
“The most interesting people you’ll find are ones that don’t fit into your average cardboard box. They’ll make what they need. They’ll make their own boxes.”
— Dr Temple Grandin